
“Take It or Leave It: The Appendix Dilemma in Endometriosis Surgery
Laparoscopic Appendectomy
Should the Appendix Be Removed During Endometriosis Surgery? What Every Patient Should Know
If you've been diagnosed with endometriosis and are preparing for surgery, your surgeon may have raised the question of whether to also remove your appendix — even if it looks completely normal. This is called a routine appendectomy, and it's one of the more debated topics in gynecologic surgery today.
This post breaks down both sides of the argument, what the medical literature actually says, and why a growing number of endometriosis specialists support removing the appendix as a standard part of the operation.
What Is a Routine Appendectomy in the Context of Endometriosis?
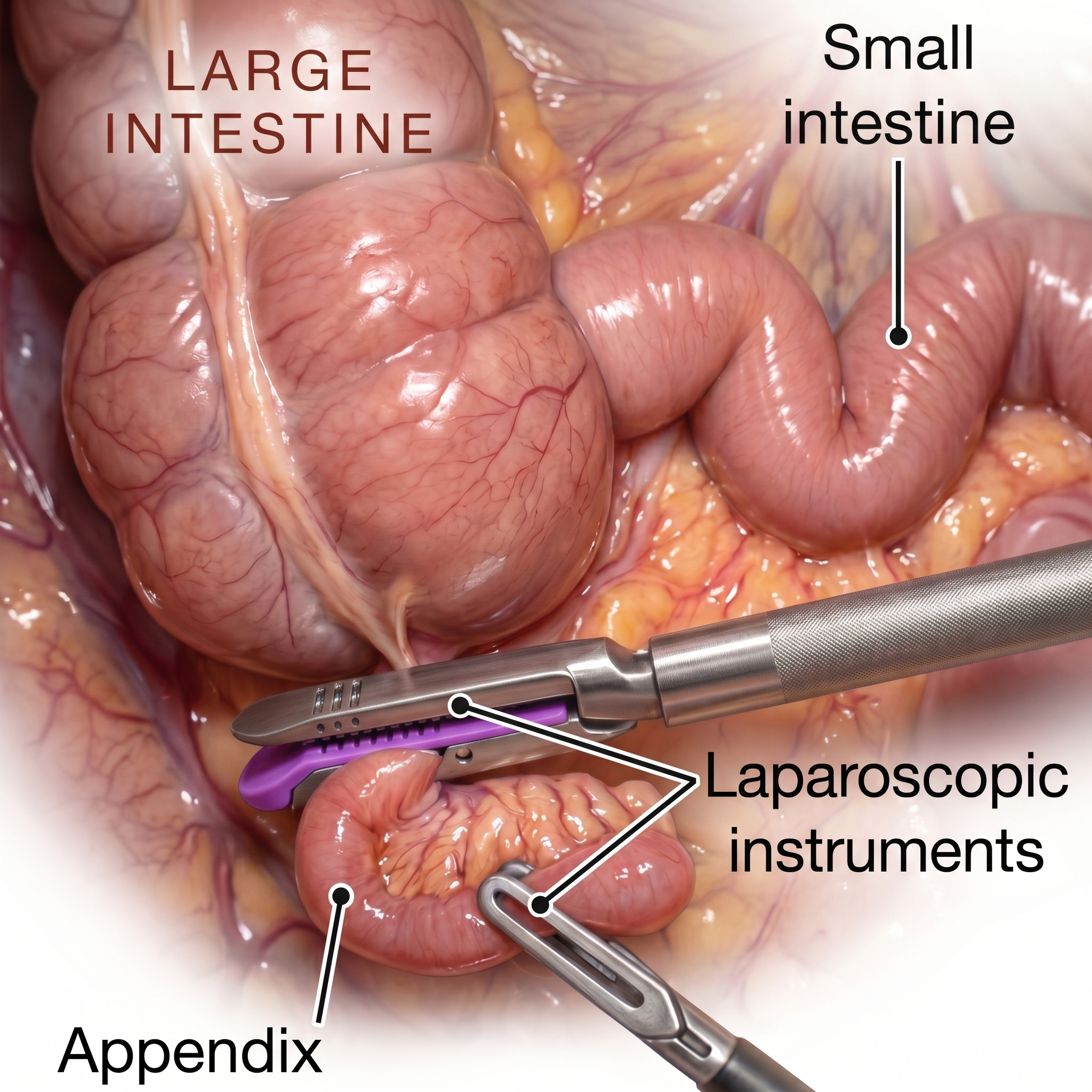
A routine or incidental appendectomy means removing the appendix during a scheduled surgery — in this case, endometriosis excision — even when the appendix doesn't appear obviously diseased. The idea is straightforward: since the surgeon is already inside the abdomen with laparoscopic instruments, why not remove an organ that is frequently involved in endometriosis and carries its own lifetime risk of appendicitis?
The appendix is located in the lower right abdomen, right where the small intestine meets the large intestine. Endometriosis lesions are drawn to this region. In fact, the appendix is one of the most commonly affected gastrointestinal sites in women with endometriosis.
How Common Is Appendiceal Endometriosis?
This is where the data gets important. Studies consistently show that the appendix is involved with endometriosis far more often than most people — and even some surgeons — realize.
A landmark study by Berker et al. (2005) published in the Journal of the American Association of Gynecologic Laparoscopists found that appendiceal endometriosis was present in approximately 13% of women undergoing surgery for endometriosis, even when the appendix looked normal to the naked eye during the procedure.
A broader systematic review by Batt and Smith (1989) identified rates ranging from 1% to 22% depending on the population studied, with higher rates in women with more advanced-stage disease.
Perhaps most striking: visual inspection during surgery is an unreliable way to detect appendiceal involvement. Endometriosis frequently infiltrates the muscular layers beneath the surface. The outside of the appendix can appear completely healthy while the inside is riddled with disease. This means that leaving the appendix behind based on how it "looks" may leave active endometriosis untreated.
The Case FOR Routine Appendectomy During Endometriosis Surgery
1. Occult Disease Is Missed by the Naked Eye
As discussed above, studies repeatedly confirm that a normal-appearing appendix can harbor endometriosis in its deeper layers. A study by Gustofson et al. (2006) in Fertility and Sterility reported that histologic confirmation of endometriosis was found in visually normal appendices removed during endometriosis surgery, supporting the argument that visual inspection alone is insufficient to rule out involvement.
2. Complete Excision Is the Gold Standard
The foundation of modern endometriosis surgery is complete excision of all visible disease. Leaving behind any endometriotic tissue — including in the appendix — risks ongoing pain, inflammation, and the need for repeat surgery. The principle of thorough excision is endorsed by major endometriosis societies, including the World Endometriosis Society (WES) and the Society of Reproductive Surgeons.
If the appendix is a known site of endometriosis, failing to remove it during an excision surgery is philosophically inconsistent with that goal.
3. Prevention of Future Appendicitis
Every woman carries a 7–8% lifetime risk of appendicitis. For women with endometriosis affecting the appendix, that risk may be compounded by the inflammatory burden of the disease itself. By removing the appendix during an already-scheduled abdominal surgery, the patient is protected from a potentially dangerous emergency surgery in the future.
Emergency appendectomy carries significantly higher complication rates than elective appendectomy. One would always prefer to remove the appendix under controlled, planned circumstances.
4. Low Added Risk When Performed by Experienced Surgeons
Critics sometimes cite surgical risk as a reason to leave the appendix alone. But the evidence doesn't support this concern when the procedure is performed in expert hands. Nezhat et al. (2010), in a study published in JSLS (Journal of the Society of Laparoendoscopic Surgeons), found that laparoscopic appendectomy added minimal operative time and did not significantly increase complication rates when performed during endometriosis surgery by skilled laparoscopic surgeons.
The appendix is typically removed in minutes. When approached laparoscopically by a surgeon experienced in advanced excision surgery, the procedure is technically straightforward.
5. Patient Quality of Life and Symptom Relief
A recurring finding in the literature is that women who had their appendix removed during endometriosis surgery reported better long-term symptom control than those who did not, particularly when the appendix was subsequently confirmed to contain endometriosis on pathology. Since pain often continues postoperatively when residual disease is left behind, removing a commonly affected organ reduces the risk of persistent or recurrent symptoms.
The Case AGAINST Routine Appendectomy
It's important to present the counterarguments honestly, because this is a genuinely debated question in the surgical community.
1. Low Prevalence Doesn't Always Justify Prophylactic Surgery
Critics argue that even if 13% of women have appendiceal endometriosis, that means 87% do not — and removing a healthy appendix in those patients offers no benefit while carrying some degree of procedural risk, including bleeding, infection, and bowel injury. The argument is essentially: don't operate on organs that aren't diseased.
2. The Appendix May Have Immunological Functions
Emerging research has suggested that the appendix may play a minor role in gut microbiome regulation and immune function. Some researchers point to population studies linking appendix removal with modest changes in gut flora and, in some cases, a slightly elevated risk of certain bowel conditions. However, it should be noted that the clinical significance of these findings remains unclear and is not universally accepted.
3. Informed Consent and Patient Autonomy
Some gynecologists feel strongly that removing any organ not confirmed to be diseased — without unambiguous pre- or intraoperative evidence — requires explicit, separate informed consent and a very clear patient-centered conversation. They advocate for a selective approach: remove the appendix only when there is a reasonable suspicion of involvement.
4. Surgical Skill Requirement
Not all endometriosis surgeons perform high-volume laparoscopic procedures, and appendectomy carries the potential for complications in less experienced hands. Some guidelines suggest that the decision should depend on surgeon experience and the complexity of the overall case.
What Do the Guidelines Say?
This is where the picture gets nuanced. As of the most recent available guidance:
The American College of Obstetricians and Gynecologists (ACOG) does not take a firm stance mandating routine appendectomy during endometriosis surgery, but acknowledges it as a reasonable consideration in appropriate clinical contexts.
The European Society of Human Reproduction and Embryology (ESHRE), in its most recent endometriosis guidelines (updated 2022), recommends surgeons consider the appendix during endometriosis surgery and notes that incidental appendectomy is justified when the appendix appears involved or when access is straightforward and risk is low.
The American Association of Gynecologic Laparoscopists (AAGL) similarly supports appendectomy during endometriosis surgery on a case-by-case basis, particularly when appendiceal involvement is suspected.
Multiple expert endometriosis excision centers advocate for routine appendectomy as standard of care when performing comprehensive excision surgery, citing the unreliability of visual inspection and the low added risk.
The takeaway: no major society currently prohibits routine appendectomy, and several support it when the conditions are right. The debate is moving in the direction of broader acceptance, particularly as surgeon experience with laparoscopic appendectomy improves.
Our Perspective: Leaning Toward Routine Appendectomy
Based on the weight of the published literature and the practical realities of endometriosis surgery, there is a strong and logical case for removing the appendix routinely when performing comprehensive endometriosis excision — particularly in the following situations:
The patient has Stage III or Stage IV endometriosis
There is any visual abnormality of the appendix, including adhesions, discoloration, or irregular texture
The patient has right-sided pelvic pain or lower right quadrant symptoms
The patient has been counseled and gives informed consent
The core logic is simple: if you are already performing a complex laparoscopic surgery to remove endometriosis from the pelvis, leaving behind a structure that is commonly involved — and that cannot be reliably cleared by visual inspection alone — is inconsistent with the goal of complete excision. When performed by a skilled surgeon, the added operative time and risk are minimal. The potential benefit — removing occult disease, preventing future appendicitis, and improving long-term symptom outcomes — is meaningful.
Key Takeaways
Appendiceal endometriosis occurs in up to 22% of women with endometriosis, and the appendix often looks normal even when affected.
Visual inspection during surgery is not reliable for ruling out appendiceal involvement.
Routine appendectomy during endometriosis surgery adds minimal risk when performed by experienced laparoscopic surgeons.
Guidelines from ESHRE and AAGL support appendectomy when involvement is suspected or when access and risk are favorable.
Many leading endometriosis excision specialists advocate for routine removal as part of comprehensive surgical care.
The decision should always involve an informed conversation between you and your surgeon.