Ovarian Endometrioma : A marker for Advanced Endometriosis ,Frequently Mismanaged

Endometrioma diagnosis ,is almost always associated with endometriosis in other places ,and sometimes even advanced endometriosis .this is what some calls the Iceberg sign .
Ovarian Endometrioma: What Patients Need to Know
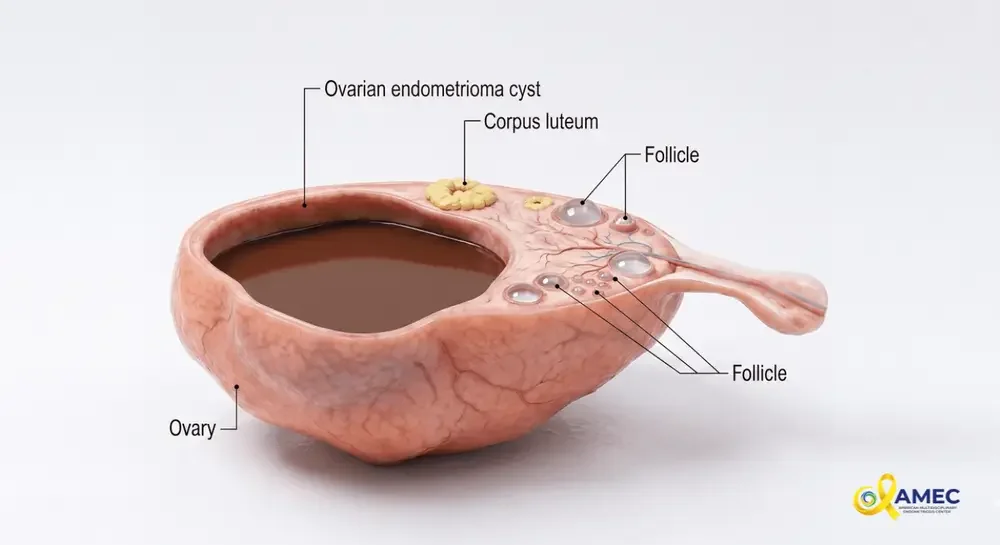
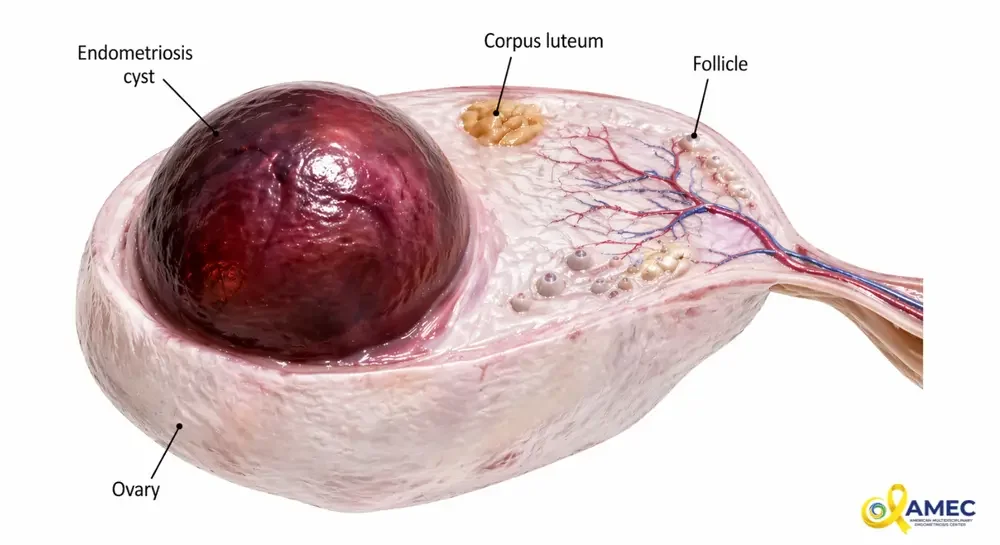
An ovarian endometrioma—often called a “chocolate cyst”—is a type of cyst that forms when endometriosis involves the ovary. These cysts are filled with old, dark blood and are one of the most recognizable forms of endometriosis on imaging. While they may appear as a single, isolated finding, ovarian endometriomas are frequently a marker of more advanced disease, often associated with deeper endometriosis affecting other pelvic structures.
Understanding what an endometrioma represents—and how it should be treated—is essential for making informed decisions about care, especially for patients concerned about pain, recurrence, and fertility.
Why Endometriomas Often Indicate Advanced Disease:
An ovarian endometrioma rarely exists in isolation. In many cases, it is part of a broader pattern of moderate to severe endometriosis, which may include:
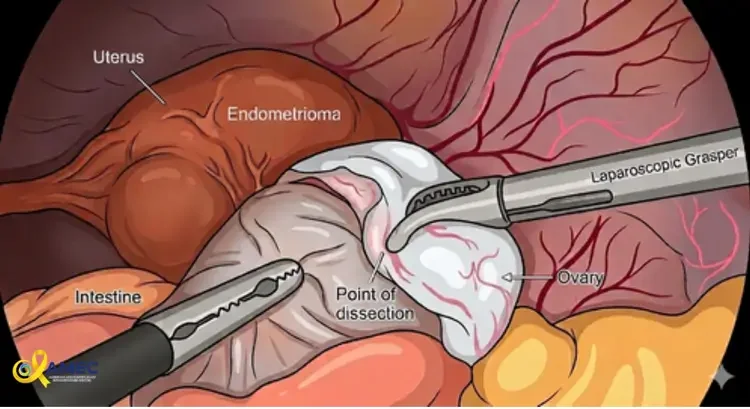
Deep endometriosis behind the uterus
Involvement of the bowel or bladder
Significant scar tissue (adhesions) distorting pelvic anatomy
Because of this, focusing only on the cyst without evaluating the entire pelvis can lead to incomplete treatment. A comprehensive surgical approach is often needed to address all areas of disease, not just the ovary.
A Common Challenge: Incomplete Management:
Ovarian endometriomas are sometimes treated by surgeons who may not specialize in advanced endometriosis. Because the cyst is visible and relatively accessible, it may be addressed in isolation, without recognizing or treating deeper disease elsewhere.
This can lead to:
Persistent or recurrent pain
Missed diagnosis of deep endometriosis
Need for repeat surgeries
For this reason, evaluation by a surgeon experienced in advanced endometriosis excision is critical, especially when imaging or symptoms suggest more extensive disease.
Treatment Options for Ovarian Endometrioma:
There are several approaches to managing endometriomas. Each has its advantages and limitations, and the choice depends on symptoms, cyst size, prior treatments, and fertility goals.
1. Drainage (Aspiration):
What it is:
The cyst is punctured and drained of its contents, often using a needle under ultrasound guidance.
Pros:
Minimally invasive
Quick recovery
Cons:
Very high recurrence rate
Does not remove the cyst wall (the source of the problem)
Bottom line:
Drainage alone is generally considered temporary and not definitive treatment.
2. Ablation (Laser or Plasma Energy)
What it is:
The cyst is opened, drained, and the inner lining is destroyed using energy sources such as laser or plasma.
Pros:
Less damage to surrounding ovarian tissue
May better preserve ovarian reserve compared to excision
Cons:
Higher recurrence rates compared to excision
May leave behind residual disease
Bottom line:
Ablation can be a reasonable option in selected patients, particularly when preserving ovarian reserve is a priority.
3. Sclerotherapy (Alcohol Treatment)
What it is:
After drainage, alcohol is injected into the cyst to destroy the lining and reduce recurrence.
Pros:
Minimally invasive
Can be performed without surgery in some cases
Cons:
Recurrence still possible
Limited ability to treat surrounding endometriosis
Less widely used as a definitive solution
Bottom line:
Sclerotherapy may be considered in select cases but is not a replacement for comprehensive surgical management when advanced disease is present.
4. Excision (Cystectomy):
What it is:
The cyst wall is surgically removed from the ovary.
Pros:
Most effective at reducing recurrence
Allows removal of the entire cyst lining
Can be combined with treatment of other endometriosis sites
Cons:
Risk of removing healthy ovarian tissue
Potential impact on ovarian reserve
Bottom line:
Excision in patient not interested in fertility is often considered the gold standard, especially when performed by an experienced surgeon who can balance complete removal with preservation of ovarian tissue.
Excision reduces cyst recurrence ,but always decrease the ovarian reserve.
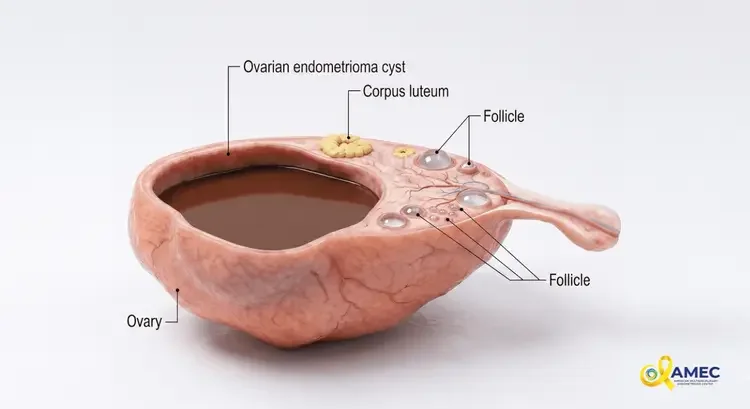
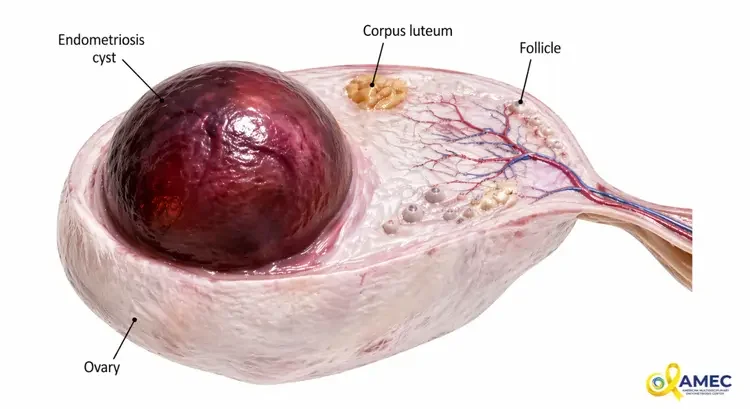
Endometrioma is also called chocolate cyst.
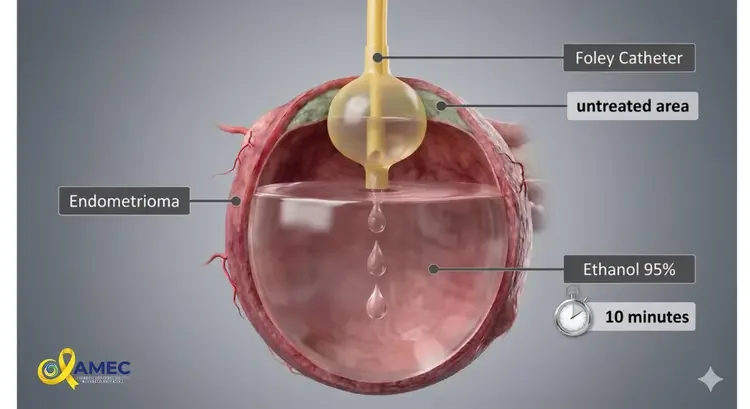
alcohol sclerotherapy is an option for patients desire future pregnancy, its less destructive on the ovary compared to excision
Balancing Treatment: Ovarian Reserve vs. Recurrence
One of the most important considerations in treating endometriomas is the balance between:
Preserving ovarian reserve (the number and quality of eggs)
Reducing the risk of recurrence and ongoing disease
Impact on Ovarian Reserve:
The ovary is a delicate organ, and any surgery carries a risk of reducing ovarian reserve. This risk depends on:
Size and location of the cyst
Surgical technique
Surgeon experience
Excision may remove some healthy tissue along with the cyst, while ablation may better preserve tissue but leave behind disease.
Risk of Recurrence:
Drainage alone → highest recurrence
Ablation/sclerotherapy → moderate recurrence
Excision → lowest recurrence
This creates a clinical trade-off that must be individualized for each patient.
Special Considerations for Patients Trying to Conceive:
For patients who want to become pregnant, treatment decisions become even more nuanced.
When Surgery May Help:
Large endometriomas interfering with ovulation
Distorted pelvic anatomy
Pain affecting quality of life
improve spontaneous pregnancy chances
improve IVF outcome.
Fertility Preservation:
IIn some cases, patients may consider:
Egg freezing before surgery
Coordinated care with a fertility specialist
The goal is to maximize chances of pregnancy while minimizing harm to ovarian reserve.
The Importance of Expertise:
Managing ovarian endometriomas is not just about removing a cyst—it’s about understanding the broader disease.
An experienced endometriosis specialist can:
Evaluate for deep and associated disease
Choose the most appropriate surgical technique
Preserve as much healthy ovarian tissue as possible
Coordinate care with fertility specialists when needed
This level of expertise is especially important in patients with recurrent cysts, severe symptoms, or fertility concerns.
Final Thoughts
Ovarian endometriomas are more than just cysts—they are often a sign of advanced endometriosis that requires careful evaluation and thoughtful management. While multiple treatment options exist, each comes with trade-offs between effectiveness, recurrence risk, and impact on fertility.
The best approach is not one-size-fits-all. It requires a personalized plan that considers symptoms, reproductive goals, and the full extent of disease. With the right expertise and a comprehensive strategy, patients can achieve better outcomes, reduce recurrence, and protect their long-term reproductive health.