
A tale of two endometriomas subtypes
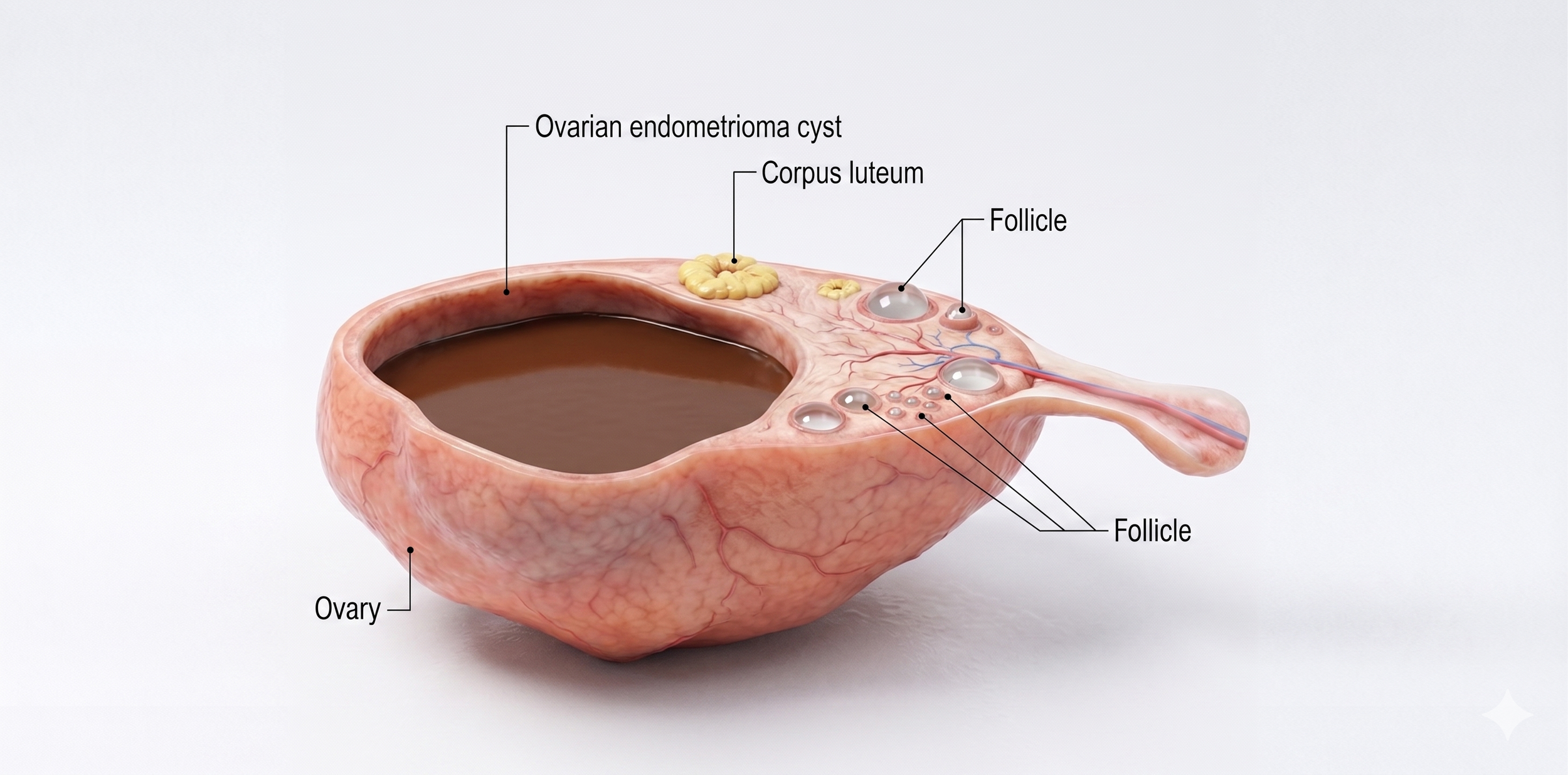
Ovarian endometrioma also known as choclate cyst
Endometriomas Explained: What Every Patient Should Know About “Chocolate Cysts”
If you’ve been diagnosed with endometriosis, you may have heard your doctor mention endometriomas—often called “chocolate cysts.” While the name may sound benign, these ovarian cysts are a significant part of the disease and can directly affect pain, fertility, and surgical outcomes.
This guide breaks down what endometriomas are, the different subtypes, and why understanding them matters for your care and future fertility.
What Is an Endometrioma?
An endometrioma is a type of ovarian cyst formed when endometriosis tissue grows on or inside the ovary. Over time, this tissue bleeds and accumulates, forming a thick, dark fluid—hence the nickname “chocolate cyst.”
But not all endometriomas are the same.
Recent surgical and pathological insights show that there are two main types, and this distinction plays a critical role in how they are treated.
The Two Types of Endometriomas
Type 1 Endometrioma (Primary)
Type 1 endometriomas are considered “true” endometriomas.
They form when endometriosis implants on the surface of the ovary, then gradually fold inward (invaginate) into the ovarian tissue.
Key Features:
Usually small (less than 2–3 cm)
Develop directly from endometriosis lesions
Very fibrotic and “sticky”
Difficult to remove surgically
No clear separation from healthy ovarian tissue
Why This Matters
Because these cysts are so tightly attached, removing them often risks removing healthy ovarian tissue along with them. This can:
Reduce ovarian reserve
Impact fertility potential
Increase surgical complexity
Type 2 Endometrioma (Secondary)
Type 2 endometriomas form in a different way.
Instead of starting on the surface, they occur when endometriosis invades an existing ovarian cyst, such as:
A follicular cyst
A corpus luteum cyst
Key Features:
Usually larger (often over 3–5 cm)
Grow within pre-existing cyst structures
Have a clearer plane of separation
Easier to remove surgically
Often allow better preservation of healthy ovary
Subtypes of Type 2
Doctors may further classify Type 2 into:
2A, 2B, and 2C, depending on how invasive or fibrotic the cyst is
This helps surgeons plan the safest and most effective surgical approach.
Why This Classification Is So Important
For patients, this is more than just medical terminology—it directly impacts:
1. Surgical Outcomes
Type 1 = higher risk of ovarian damage
Type 2 = more controlled removal
2. Fertility Preservation
Understanding the type helps your surgeon:
Minimize removal of healthy ovarian tissue
Protect egg reserve
Optimize future fertility
3. Personalized Treatment Planning
Not all endometriomas should be treated the same way. This classification allows for:
Tailored surgical techniques
Better counseling before surgery
More realistic expectations
Endometriomas and Fertility
Endometriomas can affect fertility in several ways:
Damage to ovarian tissue
Inflammation within the ovary
Reduced egg quality in some cases
Surgical removal that unintentionally reduces ovarian reserve
This is why expert surgical planning is critical—especially if you are trying to conceive now or in the future.
What Patients Should Ask Their Doctor
If you’ve been diagnosed with an endometrioma, consider asking:
What type of endometrioma do I have?
How will surgery affect my ovarian reserve?
Is surgery necessary now, or can we monitor it?
Should I consider fertility preservation (like egg freezing)?
Is my surgeon experienced in fertility-sparing endometriosis surgery?
The Bigger Picture: You Deserve Individualized Care
Endometriosis is not a one-size-fits-all disease—and neither are endometriomas.
Understanding whether your cyst is Type 1 or Type 2 can make a meaningful difference in:
Surgical success
Pain relief
Fertility outcomes
The more informed you are, the better equipped you’ll be to advocate for care that protects both your health and your future.
Final Thoughts
Endometriomas are more than just cysts—they are a reflection of how endometriosis behaves within the ovary. And with the right knowledge, they can be managed more thoughtfully and effectively.
If you take one thing away from this:
Not all endometriomas are the same—and your treatment shouldn’t be either.